


In which the doctor misdiagnoses herself
Examining the stories we tell ourselves about ourselves

Welcome to Chief Complaint! For those of you who are new, this newsletter features intermittent musings about medicine, gender, parenting, and body justice — all from your friendly neighborhood primary care doc. I’m so happy you’re here.
Well, my annual post-holiday gift is here: I am sick. The daycare germs came for us again, and it’s been a doozy.
I’ll spare you my perfect, A+ medical student version of the story (it’s too gross for Substack), but I’ll summarize.
Over Chrismukkah, my husband, son, and I all got nasty colds. I thought I was getting better, went on to host and attend several get-togethers of varying sizes, my son was on school break and getting increasingly feral with each day of unstructured mayhem, and then bam. I got even sicker.
I had some unpleasant sinus symptoms, I developed a fever — which I realized when I took my own temperature in my clinic on my way home from a day of seeing patients, womp womp — and then one of my ears started hurting.
And finally, finally, I realized what was going on.

Now, if you’re an A+ medical student — or even just an average one, like I was! — you’d know that this is a classic case of bacterial sinusitis. Like, textbook. This could be the start to a not-particularly-difficult multiple choice question.
Yet it still took me suffering for several days to realize what was happening and ask for help.
And as I sit here in my bed trying to get better, mug of tea and huge pile of tissues beside me, I’ve been reflecting on my own biases as a doctor — and as a patient. Why is it so hard to overcome the stories we tell about ourselves, and about our bodies?
As I’ve gotten more comfortable and confident as a physician in the now 7 (!) years since I graduated residency, I’ve come to think of myself as a very conservative doctor.
Not politically conservative — duh! But I do practice in a way that I call medically conservative. I try hard not to over-test my patients or over-treat my patients, and I work hard to practice medicine that’s grounded in rigorous science.
Many of my patients underestimate the harms of too many tests and getting results that may be abnormal but clinically meaningless. Or they overestimate the benefits of treatment, hoping it will fix what ails them, when in reality, the treatments aren’t as advanced as they’ve been led to believe.
Practicing conservative medicine goes against everything that’s rewarded in our corporate, capitalist health care system. This system rewards doctors who provide customer service, who act like vending machines for medications and dole out prescriptions without too many questions. It rewards doctors who give patients what they think they want, even if it harms them. It rewards quick fixes and treatments that over-promise themselves.
That’s what gets us doctors paid — not complex conversations about how to live healthier lives in a deeply unhealthy world.
I want to fight against it. I’ve taken my identity as a “conservative doctor” to heart. I truly believe it benefits my patients, but I also take pleasure in the role. I love looking up research that debunks all the waste and profiteering in modern medicine. I love commiserating with colleagues about how in primary care, less is almost always more.
How does this relate to my own little bout with illness this week? Well, antibiotics are a classic example of a mismatch between what people ask for, when in reality, they often don’t help and sometimes do harm.
To nerd out for a moment: The vast, vast majority of upper respiratory illnesses are caused by viruses, not bacteria — and they’re really hard to treat. Antibiotics don’t work, and honestly, cold and flu medicines like NyQuil don’t work either. I always tell my patients that if I had a cure for the common cold, I’d be a rich lady. I’d also be much happier in winter, with the number of daycare viruses that come through my house.
A patient “asking for antibiotics” is an ethical dilemma that we often ask medical students to explore. Here’s how the story goes: A patient has cold symptoms, and they’re convinced that antibiotics will help treat them. They badger the doctor for antibiotics, threaten to write them a bad review, or say they’ll report them to the state medical board. The doctor knows antibiotics won’t help — do they give in to the pressure?
This scenario is actually quite realistic. Just over the last week, I’ve had several conversations with patients who had classic cold symptoms who asked me to “just give them a Z-pack because that’s what the doctors at urgent care always do.”
(And as a side note, I’m always curious why patients think that antibiotics will work! I wonder if it’s because by the time they start taking the pills, their cold symptoms are starting to resolve? Or the placebo effect? I don’t doubt the power of the mind to heal the body, I’d just love to do it without awful diarrhea or antibiotic resistance.)
I had so thoroughly conceived of myself as a doctor who doesn’t dole out antibiotics for the common cold that I didn’t realize I, myself, might actually need some for an illness that actually was not the common cold.
Now, even in most cases of sinus infections, antibiotics aren’t warranted. An estimated 2% (or fewer!) are caused by bacteria. So as it started to dawn on me that this cold might be causing some unpleasant sinus symptoms, I still assumed it was viral. But as I got sicker, and I developed a fever, it became clear it wasn’t.

Luckily, the fact that it took me a few days to rewrite the narrative in my head — Mara is a hardcore doctor who practices evidence-based medicine and therefore would never be so stupid as to ask for antibiotics — didn’t have major consequences. I probably suffered a bit longer than I needed to, but ultimately, I’m okay. I got my medications. The illness isn’t very serious.
But the whole uncomfortable scenario made me start to think about my cognitive biases as a doctor — and as a human.
When I was a medical student, we had a class on differential diagnosis and cognitive bias. Differential diagnosis is the process of coming up with a list of possible causes of our patients’ symptoms, and it’s a true intellectual art. The class helped us think about different forms of bias and how they might affect our ability to land upon the correct diagnosis.
For example, anchoring bias means that doctors prioritize data that support our initial impressions — often information that’s readily available or already known. Commission bias motivates us to order a test or a treatment rather than watch and wait.
So what bias was I experiencing when I, as a doctor, was thinking about myself as a patient? The story I told myself as a powerful one: I didn’t want to think of myself as an unknowledgeable doctor. I didn’t want to think of myself as someone who, God forbid, might have to go to her own doctor. It was even a little scary to think of myself as a human with a body who needed help.
Looks like I have a lot of unlearning to do.
As an aside, there’s lots of chatter in medical circles about using AI to help doctors overcome some of these diagnostic and treatment biases.
So I plugged in my symptoms to the Doximity chatbot, and here’s what I got:
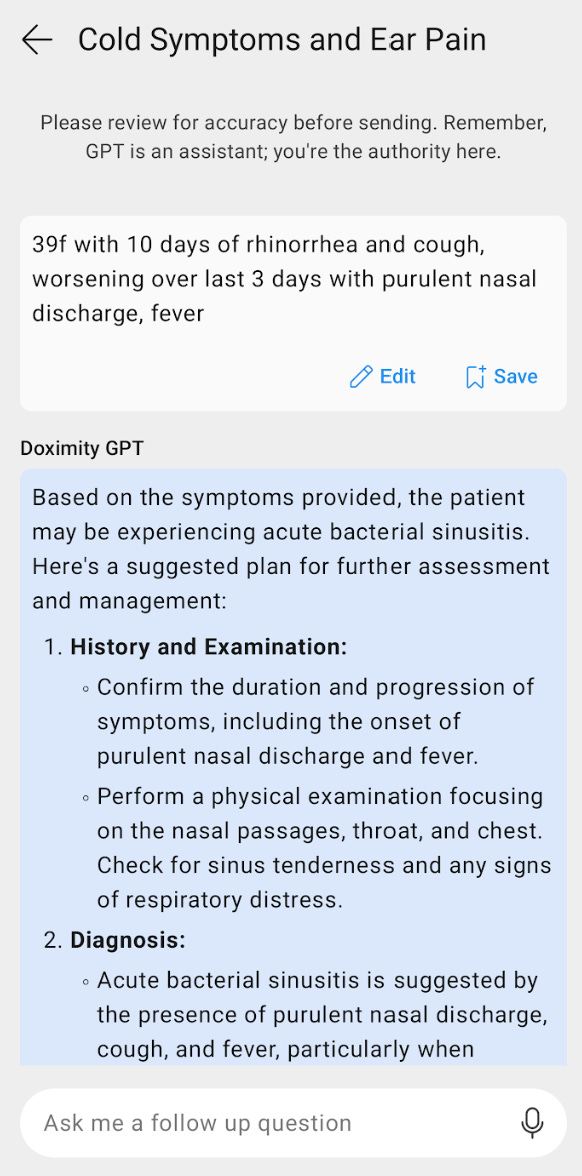
Yep, the robots are coming for my job.
Here’s another story I tell about myself: I always work while I’m sick. Even now, as I type this in bed. It’s a bad habit I picked up in medical school and residency, when I learned that to call out sick is to massively inconvenience my coworkers and patients. (Never mind that I might, uh, make them sick.) The pandemic helped me unlearn some of that nonsense, but old habits die hard.
So if you’ll excuse me, as I teach myself to tell new stories about myself, I’ll wrap this up and return to my cup of tea, My Brilliant Friend on HBO Max, and yes, my antibiotics. Happy new year, y’all.
I hope you feel better soon! Rest up. 😍
Feel better soon, Doc, and thank you for this thoughtful introspection on bias and work. It's so hard to let ourselves rest when needed, but I hope that you will.