


Why does my medical record say I'm fat?
Doctors: Don't put ob*sity in the chart. Just don't do it.

Thanks so much to my new subscribers who have arrived here by way of my latest essay for NPR. I’ve gotten so many heartening responses, and a few trolls, which I consider a badge of honor. I feel lucky to work with a thoughtful and open-minded editor at NPR.
Please read and let me know what you think.

Now, onto a topic I’ve been curious about for a while: fat stigma and the electronic medical record.
I was chatting about size-inclusive medicine with one of my medical students sometime last year, and she told me a story that stuck with me.
She had recently been to see her own primary care doctor, and she had a straightforward visit: blood pressure check, birth control prescription, check-in about her mood. The student, who was very physically active and a fan of endurance sports, hadn’t felt body shame at all. In fact, nothing about her body size or nutrition or exercise had come up in the visit.
She checked out, and she looked at the reams of paperwork she had received. (Side note: why is the paperwork you get after a doctor’s visit the health care equivalent of a CVS receipt?!)
There it was. Diagnosis: obesity.
And then pages of generic advice about “how to get to a healthy body mass index” and how to exercise more and cut calories.
The student, who presumably knows how to take care of her body appropriately for the triathlons she was fond of doing, had a good chuckle about it.
But it made me wonder what was going on. Her doctor hadn’t made her feel stigmatized or even talked about her weight at all. Yet there it was, documented as part of her permanent medical record. It’s a super specific form of medical fatphobia: doctors who don’t bring up weight during their conversation with the patient, then sneak it into the patient’s chart.

What gives? The answer, my friends, is money. It’s always money.
See, fatphobia is so deeply ingrained in the culture of medicine that obesity is not merely considered a risk factor for developing disease (which is debatable and not totally clear), it’s actually considered a disease in and of itself.
We doctors see this language everywhere, particularly around Ozempic: “Let’s de-stigmatize obesity! Treat it like the chronic disease that it is, with a medicine you take for life!”
And any disease has an ICD-10 diagnosis associated with it. What the heck is an ICD-10 diagnosis, you ask? Let’s get into the weeds a bit, here. They’re from the Medicare Bible, otherwise known as the International Classification of Diseases (Version 10).
It’s a list of everything one might possibly get diagnosed for, designed to make it easier to standardize and compare. There’s a lot in there — ranging from Z03.9, or “No Diagnosis,” to W57, “Bitten or stung by nonvenomous insect and other nonvenomous arthropods.” I use these every day, mostly by typing a few key words into the electronic medical record and clicking on the most accurate ICD-10 that pops up.
It’s mostly used for billing our patients’ insurance. It’s also used for research and, to a certain extent, actually communicating about medical decision-making with other health care providers.
Since Medicare — and frankly, most doctors — consider obesity a disease, there is absolutely an ICD-10 diagnosis associated with it. In fact, there are many different obesity-related diagnoses, for specific BMI ranges and whether or not comorbidities are associated.
And of course, the more ICD-10 codes we document, the more complex our patients appear. The more complex they appear, the more we get paid for them.
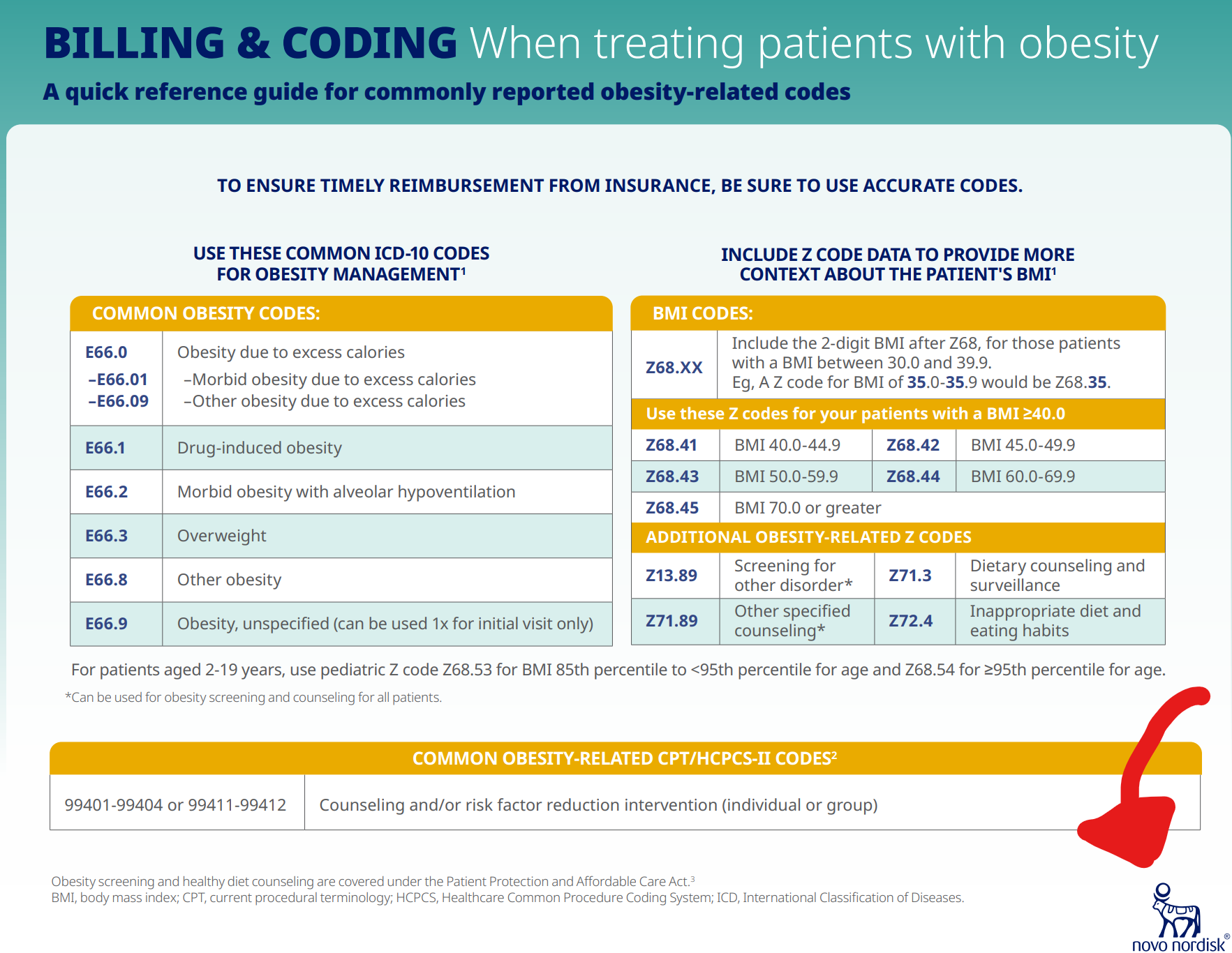
Here’s a friendly little guide to billing and coding for obesity that I found online. No wonder your doctors are eager to slap an obesity diagnosis in your medical record, even if they don’t think it’s they need to discuss in the visit.
Funny to see who created this image: check out the image in the lower right hand corner! (Psst: It’s Novo Nordisk, makers of Ozempic! Cha ching!)
For my health care wonks: it gets worse. Even deeper in the maze of health care coding and billing, we find yet another reason why doctors are eager to label their patients as “obese.” Obesity is considered a “Hierarchical Conditional Category.”
These are specific diagnoses designated by the Centers for Medicare and Medicaid Services that are supposed to estimate how “high risk” our patients are.
A doctor sneaks in an obesity diagnosis, her patient’s “risk adjustment factor” score goes up. And with certain insurers and payment models, a higher “RAF” score = more $$.
It’s relevant specifically for something called “value-based payment.” You can literally get a PhD in this, so I’ll keep it brief, but basically, insurers pay a hospital system an “up front fee” for patients based on their complexity — which, yep, is defined in part by obesity. This is in opposition to the traditional fee-for-service model, where the more frequently patients are hospitalized, the more money we make.
In value-based care, a hospital system “bets” that it will be able to make a net profit on the patient, theoretically by investing in primary care and working to keep the patient healthy and out of the hospital. Another strategy to make money for value-based care is to also invest in bureaucrats who remind primary care doctors to document HCC codes as often as possible so our patients bring in more money. “Don’t forget to code for obesity,” they say.
You can see that fat-positive doctors are up against a ton of obstacles when it comes to removing stigmatizing language from the medical record.
Still, I basically don’t document obesity any more. (There are a few exceptions, of course, since medicine is complex and there might be reasons why it’s necessary.) Not listing obesity in the chart doesn’t change the way I take care of patients, and it has the very real possibility of causing harm.
I tweeted about this approach, and of course, got a range of interesting responses.

I was glad for the discussion, and genuinely interested in the range of responses. (I kind of miss the good old days of #MedTwitter, when it was less a space for Elon Musk-style misinformation and more about sharing ideas and expertise across medical specialties, but… )
Still, we managed to have an interesting debate about this. A lot of #MedTwitter folks seemed up in arms that by not documenting obesity, we were ignoring an important risk factor for disease.
I’d argue, of course, that the link between elevated BMI and risk of early death is a lot more complicated than we acknowledge. But even if you are convinced there’s a linear relationship between BMI and the risk of disease, I still don’t think it’s necessary to document every risk factor in my patient’s chart.
Biological sex is a risk factor for certain diseases. If you’re biologically female, you’re at higher risk for breast or ovarian cancer, right? So is race — a reflection of the complex interplay of genetics, epigenetics, racism, social determinants of health, and other factors. But I don’t list my patients’ race as a diagnosis, nor their sex. Wouldn’t that be weird if your doctor did that?
So for now, my plan is to avoid all the electronic pop-ups commanding me to add obesity to my patients’ charts, avoid the glaring red BMI flag.
I’m curious: fellow size-inclusive docs, how do you address obesity in documentation? Or has anyone experienced stigmatizing language in their own medical record?
Thank you for this-- total aha moment for me! I got that ridiculous paperwork about managing my weight once after an urgent care visit for an ear infection (which I mostly thought was funny/baffling) and saw it in my chart after giving birth (which wasn't funny at all and made me think twice about my otherwise positive interaction with the triage nurse).
This is more amazing than you may even realize. I had a reasonably good PCP appointment. I allowed them to weigh me but my provider didn't mention it. However, when I went to MyChart for the visit summary it said in red all caps: the patient is ob*s*. I'd gotten through the fears about weight during the appointment only to have it in my face on my chart. :-( I dread all doctor visits because of things like this.